
Cross-specialty diagnostic integration is the process of combining diagnostic data from multiple medical specialties into a unified system to improve accuracy and collaboration in clinical decision-making. The standard industry term for this practice is integrated diagnostics, and it covers at least six domains: radiology, laboratory, pharmacy, nursing, administration, and health information systems. Healthcare professionals who understand what is cross-specialty diagnostic integration gain a direct advantage in reducing diagnostic errors, shortening time to treatment, and building more effective care teams. Tools like electronic health records (EHRs), clinical decision support systems (CDSS), and AI-powered data fusion make this integration technically possible today.
What is cross-specialty diagnostic integration, and what drives it?
Integrated diagnostics consolidates heterogeneous patient data, including radiology images, lab results, pharmacy records, and clinical notes, into a single digital framework. The goal is faster and more accurate clinical decisions, not just data storage. Rising multimorbidity is the primary driver. When a patient carries three or more chronic conditions, no single specialty has the full picture, and fragmented diagnostic pathways increase the risk of missed or late diagnoses, especially in oncology and complex care.
The shift toward integrated diagnostics is not incremental. The convergence of AI with multimodal data represents a fundamental change in how healthcare delivery is structured, moving beyond isolated specialty silos toward a coordinated, data-driven model. That shift demands both technical infrastructure and a new way of working across departments.
What are the main components and technologies behind integration?
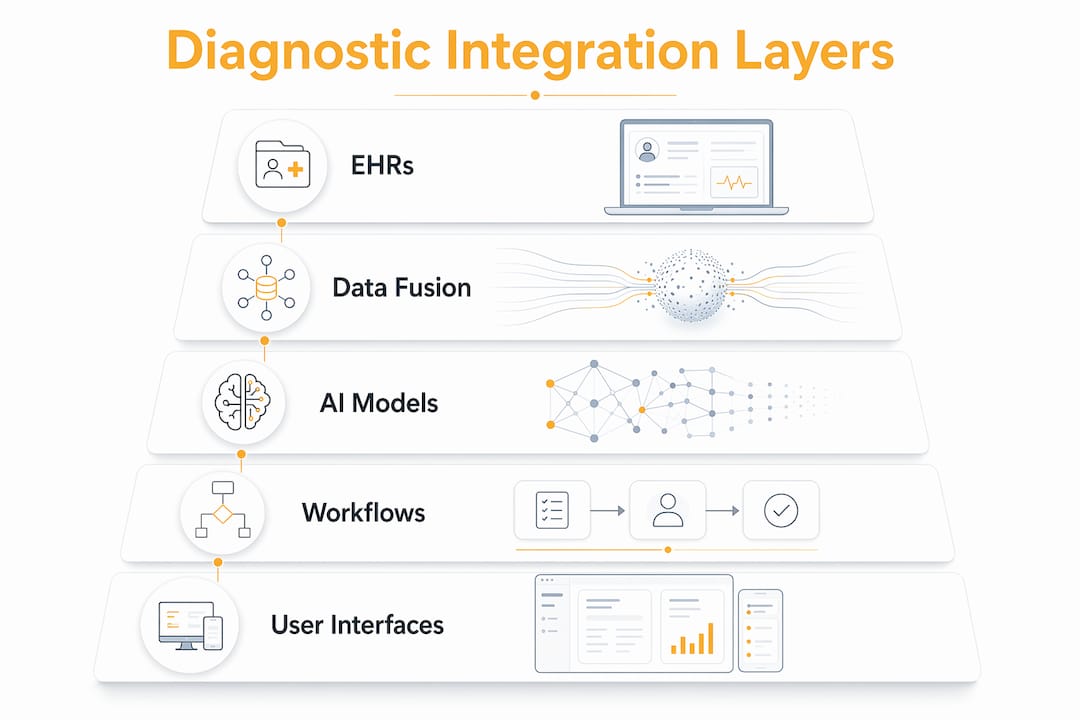
Cross-specialty diagnostic integration depends on five core technology layers working together. Each layer serves a distinct function, and gaps in any one of them degrade the whole system.

| Component | Role in integration |
|---|---|
| Electronic health records (EHRs) | Central repository connecting all specialty data streams |
| Interoperability standards (HL7, FHIR) | Enable data exchange across systems and vendors |
| Clinical decision support systems (CDSS) | Translate integrated data into real-time clinical alerts |
| AI and data fusion algorithms | Identify patterns across modalities that humans miss |
| Secure health information exchange | Protect patient privacy while enabling cross-department access |
AI models like GPT-4o show improved stability in cross-specialty diagnosis compared to earlier versions, but performance disparities among AI diagnostic models still influence the reliability of recommendations. That variability means organizations cannot treat AI as a plug-and-play solution. Selecting the right model for the right clinical context is a technical decision with direct patient safety implications.
Standardized workflows matter as much as the technology stack. Without consistent data entry protocols across radiology, nursing, and laboratory teams, even the best EHR produces fragmented outputs. Systematic diagnostic collaboration starts at the workflow level, not the software level.
Pro Tip: Before selecting an EHR or CDSS platform, map your current data entry workflows across all six integration domains. Technology built on inconsistent workflows will replicate those inconsistencies at scale.
How does integrated diagnostics improve accuracy and patient outcomes?
Multimodal diagnostic approaches outperform unimodal methods in diagnostically difficult cases. A clinical study of 863 patients across seven diseases showed that integrated approaches achieved superior diagnostic performance where single modalities failed. That finding matters because the hardest cases, the ones with the highest stakes, are exactly where integration delivers the most value.
The benefits of diagnostic integration extend across multiple clinical domains:
-
Oncology: Combining imaging, genomics, and lab biomarkers catches tumors at earlier stages and guides treatment selection more accurately than imaging alone.
-
Neurology: Integrating neuroimaging with clinical records and pharmacy data improves differential diagnosis for conditions like multiple sclerosis and early-onset dementia.
-
Cardiology: Cross-referencing ECG data, lab panels, and patient history reduces false positives in acute coronary syndrome workups.
-
Infectious disease: Merging microbiology results with pharmacy records flags antibiotic resistance patterns before they become treatment failures.
Integrated diagnostic coordination improves communication, reduces delays and errors, and enhances patient safety. The mechanism is straightforward: when a radiologist, a lab technician, and a clinician all see the same consolidated patient record, interpretive gaps close. Errors that arise from one specialist not knowing what another found are eliminated by design.
Integration tools enhance but do not replace human clinical judgment. The goal is more personalized and safer patient care, not automated diagnosis. That distinction matters for clinical teams who worry that integration means ceding control to algorithms.
What are the data fusion strategies in cross-specialty integration?
Data fusion is the technical process that makes multimodal integration work. Three architectures define how data from different specialties gets combined, and each has a specific clinical application.
-
Early fusion concatenates raw data from multiple sources before analysis. This approach suits diagnostic tasks where all data streams are available simultaneously and the relationships between them are direct.
-
Intermediate fusion leverages cross-modal latent spaces to capture spatial and contextual relationships between data types. Neuroimaging combined with clinical records uses this approach to identify structural patterns alongside symptom history.
-
Late fusion combines predictions from separate models rather than raw data. This approach suits prognostic tasks, such as predicting disease progression, where each specialty’s model contributes an independent probability estimate.
Matching fusion type to clinical goals is a prerequisite for effective integration. A late fusion model applied to a diagnostic task will underperform because it discards the raw signal relationships that early or intermediate fusion preserves. Misaligned fusion choices degrade diagnostic effectiveness in ways that are hard to detect without rigorous validation.
| Fusion type | Best clinical use | Risk if misapplied |
|---|---|---|
| Early fusion | Diagnosis with simultaneous data | Noise amplification from poor-quality inputs |
| Intermediate fusion | Spatial or contextual diagnosis | Computational complexity, interpretability loss |
| Late fusion | Prognosis, risk stratification | Loss of cross-modal signal in diagnostic tasks |
Pro Tip: Define your clinical goal first: diagnosis or prognosis. That single decision determines which fusion architecture to build toward. Choosing architecture before defining the goal is the most common technical mistake in integration projects.
What challenges do healthcare organizations face in implementing integration?
Implementation challenges fall into three categories: technical, cultural, and ethical. Most organizations underestimate the cultural and ethical dimensions.
-
Interoperability gaps: Legacy systems often use proprietary data formats that resist HL7 or FHIR standards. Retrofitting these systems is expensive and time-consuming.
-
Cultural resistance: Radiologists, laboratory scientists, and clinicians have historically operated in separate professional cultures. Full integration demands cultural change for interdisciplinary coordination, not just technical connectivity.
-
AI explainability: Clinicians distrust black-box AI. Explainability tools like SHAP and Grad-CAM are critical for gaining clinical trust and enhancing interpretability of multimodal models. Without them, adoption stalls regardless of model accuracy.
-
Privacy and security: Consolidating data across six domains multiplies the attack surface for breaches. Governance frameworks must address consent, access controls, and audit trails from day one.
-
Workflow standardization: Real-time cross-department communication requires agreed-upon data entry standards. Organizations often fail by focusing on IT alone and neglecting workflow and cultural factors.
Cross-specialty integration requires ethical and systemic consideration, including bias mitigation and privacy protection. AI models trained on non-representative datasets will produce biased recommendations, and integrated systems amplify that bias across all connected specialties.
Pro Tip: Run a cultural readiness assessment alongside your technical audit. Survey department heads in radiology, laboratory, nursing, and administration about their current cross-department communication practices. The gaps you find there predict implementation friction more accurately than any IT audit.
How can healthcare providers implement cross-specialty integration practically?
Practical implementation follows a defined sequence. Skipping steps creates technical debt that compounds over time.
-
Assess current state. Audit all diagnostic data sources across radiology, laboratory, pharmacy, nursing, and administration. Identify format inconsistencies, access barriers, and communication gaps between departments.
-
Select interoperable technology. Choose EHR and CDSS platforms that support HL7 FHIR standards natively. Platforms like MESI mTABLET demonstrate how integrated point-of-care tools can consolidate multiple diagnostic streams at the clinical encounter level.
-
Engage stakeholders early. Include radiologists, laboratory directors, nursing leads, and IT security officers in the design phase. Decisions made without their input get reversed during rollout.
-
Redesign workflows before deployment. Standardize data entry protocols across all departments. Define who enters what, when, and in what format, before the system goes live.
-
Deploy AI-enhanced analytics with explainability built in. Use models that incorporate SHAP or Grad-CAM outputs so clinicians can interrogate recommendations. Accuracy without explainability does not translate to adoption.
-
Train interdisciplinary teams continuously. Integration is not a one-time deployment. Schedule quarterly cross-department reviews to identify workflow drift and retrain staff on updated protocols.
AI-enhanced analytics for decision support work best when clinical teams understand what the models are doing. Training that covers both the technical outputs and the clinical interpretation of those outputs produces faster adoption and fewer override errors.
Key takeaways
Cross-specialty diagnostic integration delivers its greatest value when technical architecture, clinical workflow, and interdisciplinary culture are aligned from the start.
| Point | Details |
|---|---|
| Integration spans six domains | Radiology, laboratory, pharmacy, nursing, administration, and health information systems must all connect. |
| Fusion strategy must match clinical goal | Early fusion suits diagnosis; late fusion suits prognosis. Mismatches degrade performance. |
| Cultural change is non-negotiable | IT interoperability alone does not produce integration. Workflow and team coordination must change too. |
| AI explainability drives adoption | Tools like SHAP and Grad-CAM are prerequisites for clinician trust, not optional add-ons. |
| Multimorbidity makes integration urgent | Fragmented pathways increase missed diagnoses in complex patients. Integration closes that gap. |
Why I think most integration projects fail before they start
The organizations I have watched struggle with integrated diagnostics share one pattern: they treat it as an IT project. They buy the EHR, configure the FHIR endpoints, and then wonder why radiologists and laboratory directors are still emailing each other PDFs six months later.
The research is clear. Successful integration requires interdisciplinary coordination that goes well beyond technical connectivity. The cultural gap between a radiologist who has spent 20 years reading films independently and a clinical team that wants real-time input on a shared dashboard is not solved by software. It is solved by leadership that treats cross-specialty collaboration as a clinical priority, not an IT deliverable.
The AI dimension adds another layer of complexity that most implementation plans underestimate. Clinicians do not adopt tools they cannot explain to a patient or a peer review board. SHAP and Grad-CAM outputs are not just technical features. They are the difference between a model that gets used and one that gets bypassed. Any integration roadmap that does not include explainability as a core requirement is incomplete.
My honest view is that the organizations getting this right are the ones that started with a clinical question, not a technology selection. They asked, “Where are our diagnostic errors concentrated?” and then built the integration architecture around answering that question. That sequence produces better outcomes and faster adoption than any vendor-led implementation I have seen.
— Amy
How Kohealthlabs supports integrated clinical diagnostics
Kohealthlabs was built specifically to address the fragmentation that makes cross-specialty integration so difficult in clinical research settings. By consolidating central laboratory services and radiology under a single contract, Kohealthlabs eliminates the vendor coordination burden that slows CROs, government agencies, and wellness programs.
The platform delivers structured, analysis-ready data bundles that combine over 100 biomarkers with advanced AI analytics. AI identifies protocol deviations, supports regulatory compliance, and accelerates trial timelines without requiring clinical teams to manage multiple data pipelines. For organizations building toward integrated clinical diagnostics, Kohealthlabs provides the infrastructure to make that transition practical and auditable from day one.
FAQ
What is cross-specialty diagnostic integration in simple terms?
Cross-specialty diagnostic integration combines data from radiology, laboratory, pharmacy, nursing, and administration into one unified system. The goal is faster, more accurate clinical decisions by giving all specialists access to the same complete patient record.
How does integrated diagnostics reduce diagnostic errors?
Integrated diagnostic coordination improves communication across departments and eliminates interpretive gaps that arise when specialists work from incomplete information. Research shows it reduces delays and errors while enhancing patient safety.
What is the difference between early, intermediate, and late fusion?
Early fusion combines raw data before analysis and suits diagnostic tasks. Intermediate fusion captures cross-modal relationships and suits spatial diagnosis. Late fusion combines model predictions and suits prognostic tasks like disease progression forecasting.
Why do AI models need explainability tools in integrated diagnostics?
Clinicians distrust black-box AI recommendations they cannot interrogate. Explainability tools like SHAP and Grad-CAM make model outputs interpretable, which is a prerequisite for clinical adoption rather than an optional feature.
What is the biggest barrier to implementing cross-specialty integration?
The biggest barrier is cultural, not technical. Organizations that focus only on IT interoperability and neglect workflow standardization and interdisciplinary coordination consistently fail to achieve functional integration.